When I look through the various published studies examining how effective exercise protocols are for rehabilitating shoulder instability, I can’t help but notice the wide range of exercises used: neuromuscular control, closed kinetic chain, isometric, heavy resistance, light resistance, Watson protocol, Rockwood protocol, …. Why are there so many? Does it need to be that complicated?
Past rehab protocols
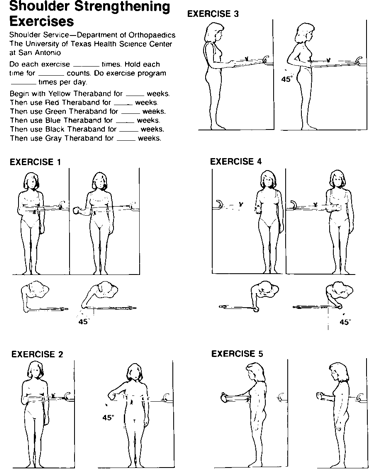
When I started as a physiotherapist in 2008, we used the Rockwood protocol (figure 1). The Rockwood protocol includes a series of simple resistance band exercises. Patients were instructed to focus on holding their shoulder blades down and back to “stabilise” their shoulders.
In 2013, a group of the world’s leading shoulder injury researchers got together to reach a consensus on shoulder blade positioning’s role in shoulder injuries. The good news for people with hypermobile shoulders was that the group concluded that shoulder stability was more about the muscle action, or dynamic joint stability, than joint capsule stiffness, or passive joint stability.[1]
However, the bad news was they admitted they really didn’t know why strengthening the muscles didn’t consistently improve shoulder stability. The researchers also suggested that shoulders being rolled too far forward may be part of the problem. The conclusions reached from this consensus supported the use of the Rockwood protocol.
Perhaps based on the lack of consistent success from the Rockwood protocol, in 2016-2017, it was discovered that if patients used more complicated shoulder movements with the Watson protocol, they had greater improvements in their shoulder stability than if they used the Rockwood protocol.[2,3]
The Watson protocol built on the Rockwood protocol by incorporating the use of a resistance band around the shoulder to cue the person to hold their shoulder blade back and performing more exercises with an elevated arm. An example of one of the Watson protocol exercises is shown in figure 2.
At the same time as the Watson protocol was being recommended by some academics, the theories on the “correct” movement of the shoulder blade for shoulder exercises was being questioned by other academics.[4] These other researchers proposed that bringing more of the body into the shoulder exercises may better facilitate the shoulder blade and shoulder muscles to work than holding the body in a rigid state.[5,6,7,8]

Hunter-Gatherer Design
I agree with the researchers who recommend bringing the whole body into the shoulder exercises. I really started to question the concept of “stabilizing” the shoulder blade in a rigid way, as was promoted in the Rockwood and Watson protocols, when I had multiple hypermobile patients report shoulder dislocations that resulted from the person trying to “stabilize” their shoulder blade while they reached forward. In hindsight, it seems so unnatural to try and pull your shoulder blade down and back while you try to lift your arm up and forward.
From the perspective of what is natural for the shoulder, I draw inspiration from the theories of evolutionary medicine. Evolutionary medicine is the field of medicine that applies the principles of evolutionary biology to health and disease.[9] In the case of how a shoulder moves, evolutionary medicine would think of how the shoulder’s function had been honed over 300,000 years resulting in the hunter-gatherer design. This hunter-gatherer design is the body we inhabit today. From this perspective, when it comes to restoring healthy shoulder function by prescribing movements within the design of the shoulder, I ask myself a simple question, “would a hunter-gatherer use this movement pattern?”
Further, when it comes to how heavy the resistance for the exercises should be, I wonder, would a hunter-gather have needed to lift that heavy? Researchers at The University of Southern Denmark looked at people with hypermobile spectrum disorder (HSD) with shoulder pain and instability lasting greater than 3 months and compared the benefits of 16 weeks of “heavy” strength training to “light” strength training. They found that light and heavy resistance were equally as effective at reducing shoulder pain and restoring shoulder function, but heavy resistance had some additional mood boosting benefits. So, heavy resistance is great, but you don’t need it to improve shoulder stability.
If we don’t need heavy weights, resistance bands looped over our shoulders, or a robot-like rigid posture, what exercises do we need to improve shoulder stability?
I discuss the principles of improving joint control here.
To briefly recap, researchers have found that you can improve your body awareness and control (or proprioception) with practice.[10,11,12,13] The elements of practice that help improve body awareness include:
- Mental focus on the movement you hope to improve
- Visual, auditory, and or touch feedback (to confirm the movement has been performed as expected)
- Movement specificity (improvement is specific to speed, angle, load, and whether it is an open or closed kinetic chain movement)
- Reward (achieving the objective activates reward circuitry in the brain which reinforces the “rewiring” in the brain)
- Frequency (the more you practice the better you get)
A helpful example
To help this information make sense, let me give you an example of how I might prescribe shoulder stabilisation exercises.
A common case I will see in the hypermobile community is a person with years of progressively more frequent shoulder pain, popping, clicking and trouble performing activities of daily living. There was no initiating traumatic injury, it gradually set in for a combination of reasons. The shoulder can be a problem randomly with a wide range of activities including with sleep positions. So, the aim of rehabilitation is general shoulder movement, as opposed to a specific action, like throwing.
A common exercise routine I prescribe for restoring shoulder stability in the aforementioned cases is this tai chi YouTube video. I know what you’re thinking, hunter-gatherers didn’t do tai chi. The reason I chose this video is because it is a simple, accessible, and an affordable way to gradually build shoulder control over a wide range of movements in a gentle way.
Even though it is only a seven-minute routine, I still recommend a graduated approach. For examples, my patient and I might outline the following plan:
- To improve my joint stability, I am going to try this tai chi routine, checking my technique in a mirror
- I will practice tai chi on Wednesday and Saturday
- On the first Wednesday, I’ll limit the size of the movements to about 50% of those demonstrated in the video and only try the first half of the video
- If I don’t “pay for that” with an increase in my symptoms of over 20%, and my symptoms are back to “normal” by Saturday, I’ll perform 50% of the tai chi routine at 50% range of motion again
- Assuming I am back to my usual level of discomfort by the next Wednesday, I will perform the movements to about 75% of the demonstrated size
- If the 75% range of motion was well tolerated, I repeat 75% range on Saturday
- If the 75% range of motion is well tolerated once again, I will perform the full range of motion demonstrated in the tai chi video on Wednesday
- I will then add the next movement pattern on the video at 100% movement range
- I will continue to add one movement pattern per week until I am performing the full video at full range of motion
- I then continue this same routine until I feel ready for a greater challenge
- I hope to notice some improvement in my physical discomfort after six weeks
Give it a try for yourself and see what you think.
- Kibler, W. B., Ludewig, P. M., McClure, P. W., Michener, L. A., Bak, K., & Sciascia, A. D. (2013). Clinical implications of scapular dyskinesis in shoulder injury: the 2013 consensus statement from the ‘Scapular Summit’. British journal of sports medicine, 47(14), 877–885. https://doi.org/10.1136/bjsports-2013-092425
- Watson, L., Warby, S., Balster, S., Lenssen, R., & Pizzari, T. (2016). The treatment of multidirectional instability of the shoulder with a rehabilitation program: Part 1. Shoulder & elbow, 8(4), 271–278. https://doi.org/10.1177/1758573216652086
- Watson, L., Warby, S., Balster, S., Lenssen, R., & Pizzari, T. (2017). The treatment of multidirectional instability of the shoulder with a rehabilitation programme: Part 2. Shoulder & elbow, 9(1), 46–53. https://doi.org/10.1177/1758573216652087
- McQuade, K. J., Borstad, J., & de Oliveira, A. S. (2016). Critical and Theoretical Perspective on Scapular Stabilization: What Does It Really Mean, and Are We on the Right Track?. Physical therapy, 96(8), 1162–1169. https://doi.org/10.2522/ptj.20140230
- Barramuño-Medina, M., San Martín-Zurita, S., Silva-Correa, V., Téllez-Camilo, T., Valdés-Badilla, P., Bascour-Sandoval, C., & Gálvez-García, G. (2025). Kinetic chain modifies muscle activation in adults with shoulder pain: a randomized cross-over trial. Journal of shoulder and elbow surgery, 34(6), e468–e476. https://doi.org/10.1016/j.jse.2024.10.023
- Nagai K, Tateuchi H, Takashima S, Miyasaka J, Hasegawa S, Arai R, et al. Effects of trunk rotation on scapular kinematics and muscle activity during humeral elevation. J Electromyogr Kinesiol 2013;23: 679-87. https://doi.org/10.1016/j.jelekin.2013.01.012
- Richardson E, Lewis JS, Gibson J, Morgan C, Halaki M, Ginn K, et al. Role of the kinetic chain in shoulder rehabilitation: Does incorporating the trunk and lower limb into shoulder exercise regimes influence shoulder muscle recruitment patterns? Systematic review of electromyography studies. BMJ Open Sport Exerc Med 2020;6:1-12. https://doi.org/10.1136/bmjsem-2019-000683
- Yamauchi T, Hasegawa S, Matsumura A, Nakamura M, Ibuki S, Ichihashi N. The effect of trunk rotation during shoulder exercises on the activity of the scapular muscle and scapular kinematics. J Shoulder Elbow Surg 2015;24:955-64. https://doi.org/10.1016/j.jse.2014.10.010
- Grunspan, D. Z., Nesse, R. M., Barnes, M. E., & Brownell, S. E. (2017). Core principles of evolutionary medicine: A Delphi study. Evolution, medicine, and public health, 2018(1), 13–23. https://doi.org/10.1093/emph/eox025
- Aman, J. E., Elangovan, N., Yeh, I. L., & Konczak, J. (2015). The effectiveness of proprioceptive training for improving motor function: a systematic review. Frontiers in human neuroscience, 8, 1075. https://doi.org/10.3389/fnhum.2014.01075
- Han, J., Waddington, G., Adams, R., Anson, J., & Liu, Y. (2016). Assessing proprioception: A critical review of methods. Journal of sport and health science, 5(1), 80–90. https://doi.org/10.1016/j.jshs.2014.10.004
- Rossi, C., Bastian, A. J., & Therrien, A. S. (2021). Mechanisms of proprioceptive realignment in human motor learning. Current Opinion in Physiology, 20, 186-197. https://doi.org/10.1016/j.cophys.2021.01.011
- Therrien, A. S., & Wong, A. L. (2022). Mechanisms of Human Motor Learning Do Not Function Independently. Frontiers in human neuroscience, 15, 785992. https://doi.org/10.3389/fnhum.2021.785992