
In 2005, I was working as a physiotherapy student clinician in a rehabilitation clinic and my supervisor told me the client’s leg pain was coming from their back. I was baffled, how was that possible? How could their leg pain be back pain? It was leg pain! My supervisor went on to explain “sciatica.” She said sciatica is referred pain and referred pain happens throughout our body, such as when people feel left arm pain while having a heart attack.
I later learned that we don’t only experience referred pain, we also experience other referred sensations. In 2008, I was learning about a headache treatment and my mentor pressed on my upper neck and I felt head pain, dizziness, nausea, and visual disturbance. It was so weird, I didn’t have any problems before she pressed on my neck and as soon as she stopped pressing the sensations went away.
I was so fascinated, how and why do we experience referred sensations?
How
Scientists propose that we experience referred sensations (or referred symptoms) due to something called “convergence.” Convergence is when nerves carrying signals from one part of the body meet up with nerves carrying signals from another part of the body and beyond the meeting point the signal flows along a common channel (Figure 1).
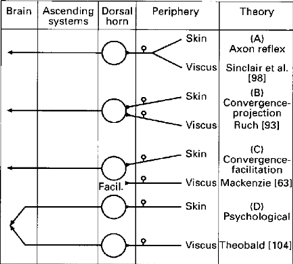
Figure 1. the various theoretical types of nerve convergence (McMahon, 1995, p. 134, taken from Morrison, 1987)
Once the signal reaches the parts of the brain responsible for interpreting where the signal originally came form, the brain decides it came from the most innervated and sensitive area.
When it comes to neck muscle tension referring pain into the head, the point of convergence is the trigeminal nerve nucleus located in the spinal cord and the brain stem. [3,4] This process of neck pain referring to the head is explained well in this brief YouTube video by Physiotutors.
When it comes to neck muscle tension causing dizziness, visual disturbance, and nausea, the convergence occurs in areas of the brain called the vestibular nuclei, thalamus, cerebellum, reticular formation, and cerebral cortex. [5]
Why?
Our eyes see, our muscles move, and our vestibular system enables us to stay upright. Our ability to walk over to a piece of fruit, pick it up, and bring the fruit to our mouth depend on our eyes, muscles, and vestibular systems working together.
To work together, our muscles, eyes, and vestibular system need to talk and to talk their signals need to converge. In other words, our ability to interact with the world depends on “multisensory integration.” The upside to multisensory integration is we can throw, catch, run and jump; the down side to multisensory integration is referred symptoms.
What can you do?
Neck dysfunction causing your symptoms (or “cervicogenic” symptoms) is a diagnosis of exclusion. In other words, when doctors rule out all other causes of your symptoms, they decide your neck may be the cause. I discuss some of the other causes of cooccurring head pain, dizziness, visual disturbance and nausea in this blog post and this blog post.
So, if your doctor thinks you may have cervicogenic head symptoms, it might be worth trying treatments that help the muscles in your upper neck relax and trying exercises that improve your neck movement and control. In my experience, different people respond to different treatments. Some people respond well to massage, some to joint mobilisation, some respond to acupuncture, some to exercise, some to injection therapies, and others to some combination of the aforementioned. I have even seen some people how respond to the use of a neck brace for periods of the day to help their neck muscles relax. I suggest you consult your doctor if you suspect your neck may be contributing to your symptoms. If you and your doctor agree that neck muscle treatment is worth trying, start with the option you feel most comfortable with and go from there.
- McMahon, S & Dmitrieva, Natalia & Koltzenburg, M. (1995). Visceral pain. British journal of anaesthesia. 75. 132-44. 10.1093/bja/75.2.132.
- Morrison JFB. Sensations arising from the lower urinary tract. In: Torrens M, Morrison JFB, eds. The Physiology of the Lower Urinary Tract. Berlin: Springer-Verlag, 1987; 89–132.
- Fernandes EC, Carlos-Ferreira J, Luz LL, Safronov BV. Presynaptic Interactions between Trigeminal and Cervical Nociceptive Afferents Supplying Upper Cervical Lamina I Neurons. J Neurosci. 2022 Apr 27;42(17):3587-3598. doi: 10.1523/JNEUROSCI.0025-22.2022. Epub 2022 Mar 22. PMID: 35318285; PMCID: PMC9053849.
- Johnston, M. M., Jordan, S. E., & Charles, A. C. (2013). Pain referral patterns of the C1 to C3 nerves: implications for headache disorders. Annals of neurology, 74(1), 145-148.
- De Hertogh, W., Micarelli, A., Reid, S., Malmström, E. M., Vereeck, L., & Alessandrini, M. (2025). Dizziness and neck pain: a perspective on cervicogenic dizziness exploring pathophysiology, diagnostic challenges, and therapeutic implications. Frontiers in neurology, 16, 1545241. https://doi.org/10.3389/fneur.2025.1545241



